A substantial amount of research has been undertaken to understand and measure adherence to treatment in asthma. In most OECD countries the average is half of adults take their medication at least 80% of the time (Bender & Rand 2004). In Australia adherence ranges from 40-70% (Franks et al. 2005) and in pregnant women adherence is in the higher range at 60% (Murphy et al. 2005). Analysis from surveys taken in 2012 showed significant decreasing use of preventer medications in pregnant women with asthma and a worrying trend for increased reliever use (Sawicki et al. 2012).
The lack of adherence may reflect an intentional non-adherence as research has found 82% of females had concerns about ICS affecting their fetus. Other research demonstrated that pregnant women desired further information about inhaled medications (Chambers 2003). Suboptimal adherence has been overwhelmingly linked to worsening outcomes for people with asthma and the risks to the pregnant woman and the fetus can be extremely serious (Murphy et al. 2005)

Adherence needs to be assessed in a non-judgemental manner and be integral to asthma assessment and follow up. Several methods can be employed such as asking open-ended questions “do you miss many doses of your preventer” or “do you find it hard to pay for your medications”. Nearly all preventer inhalers in Australia are fitted with a dose counter, this can be examined and enquired as to when the inhaler was commenced giving a number of prescribed activations versus how many were recorded by the device. Prescription records can provide information on how many inhalers have been dispensed, though decentralised records in Australia can make this difficult to access (Holmes & Heaney 2021). The recent development of electronic monitoring devices (EMD) that can be attached to inhaled medications devices allows for objective adherence monitoring. EMDs have been shown to improve adherence, however their use is not widespread outside of research (Lee et al. 2021).
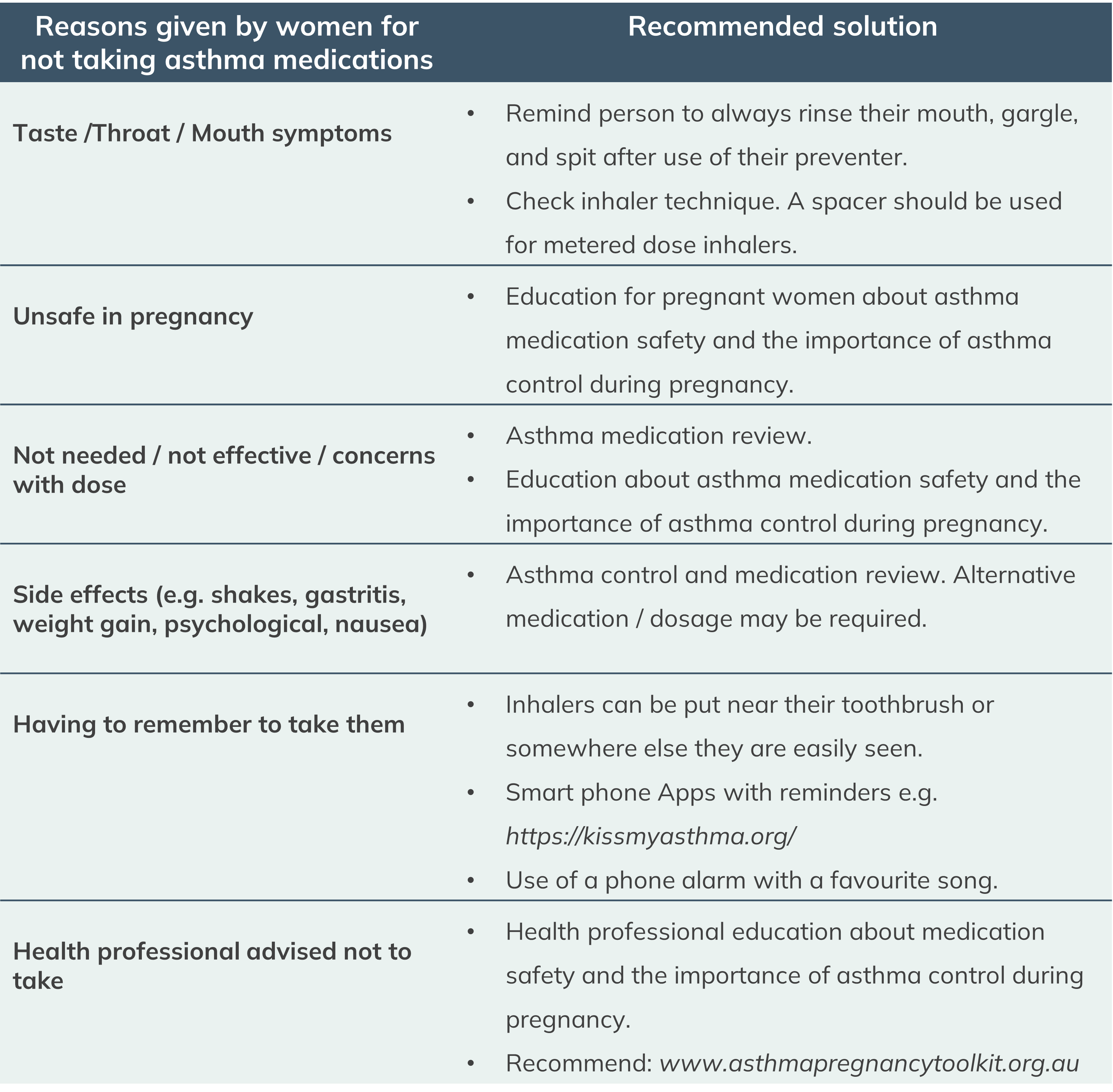
If sub optimal adherence and/or challenges to adherence are identified, strategies to mitigate and assist the patient must be employed. A simple discussion with the woman that focuses on the benefits of adherence and the risks of sub optimal adherence can be beneficial (Foster et al. 2014). Reducing the number of inhalers can improve adherence and reduce costs. Finally understanding the reasons for sub optimal adherence will allow you to tailor the intervention to the patients’ needs. Some common intentional and non-intentional reasons for non-adherence during pregnancy and measures to address these, are listed below (Murphy et al. 2022):
View a webinar on Inhaler Use from the Centre of Excellence in Severe Asthma.